Abstract
Background: Early detection of arterial damage is essential for the primary prevention of complications linked to type 2 diabetes (T2D). The study assessed the cardiovascular risk of sub-Saharan African individuals with T2D, while exploring possible mechanisms involved in the pathogenesis of vascular complications in this population. Methodology: A crossover study of 72 sub-Saharan African adults (36 with T2D and 36 without T2D) was conducted. Outcomes including diameter size (mm) and blood velocity (cm/s) of the brachial artery, were obtained at seven time points: baseline and from 5 seconds to 600 seconds in two conditions: pre- and post Nitric Oxide (NO) administration. HbA1C, fasting glucose, age, BMI, mean arterial pressure (MAP), lipid profile, T2D duration since diagnosis, and binary indicators of insulin and oral diabetes medication were evaluated. Results: NO improved the blood flow compared to the pre-NO after adjustment for clinical factors. The beneficial effect of NO administration on vascular dynamics was influenced by age (B=1.09; 95%IC: 1.07, 1.11), increased BMI (B= 1.03; 95%IC: 1.01, 1.04) and insulin use (B = 1.13; 95%IC 1.10, 1.16). Conclusion: The nuanced impact of these factors on blood flow improvement related to NO necessitates tailored and personalized approaches in managing T2D patients.
Keywords
Type 2 Diabetes, Cardiovascular Risk, Vascular Dynamics, Sub-Saharan Africa
1. Introduction
Type 2 diabetes (T2D) stands as a persistent global health challenge, marked by its chronic nature and widespread prevalence. Classified as a true pandemic, estimates from the International Diabetes Federation (IDF) in 2013 indicated that approximately 400 million individuals worldwide were afflicted by diabetes, with 80% of this burden concentrated in low- and middle-income countries
. Of particular concern is the African continent, where T2D has entrenched itself, demonstrating a prevalence of 6-10% in Sub-Saharan Africa in 2014, and projections suggest this figure may rise to 41 million individuals by 2035
| [3] | Mbanya, J. C., Motala, A. A., Sobngwi, E., Assah, F. K., Enoru, S. T., & Diabetes in Sub-Saharan Africa Study Group. (2014). Diabetes in sub-Saharan Africa. The Lancet, 383(9933), 1009–1020. https://doi.org/10.1016/S0140-6736(13)62189-7 |
| [4] | World Health Organization. (2014). Global status report on noncommunicable diseases 2014. Retrieved from https://www.who.int/nmh/publications/ncd-status-report-2014/en/ |
[3, 4]
. Contributing factors to this surge include the aging demographic and increasing urbanization, both of which are conducive to the epidemiological expansion of diabetes
| [5] | Emerging Risk Factors Collaboration. (2010). Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. The Lancet, 375(9733), 2215–2222. https://doi.org/10.1016/S0140-6736(10)60484-9 |
[5]
.
Type 2 diabetes (T2D) has emerged as a global health challenge, reaching pandemic proportions, particularly in low- and middle-income countries. The African continent, with a significant portion of its population residing in Sub-Saharan regions, faces a substantial burden of T2D. The present study sought to investigate the prevalence of vascular complications among individuals with T2D in Sub-Saharan Africa and explore potential mechanisms contributing to the pathogenesis of these complications.
The onset of T2D is intricately linked to insulin resistance, a precursor that leads to hyperinsulinism and an impaired utilization of blood glucose by the body's cells. This cascade sets the stage for chronic hyperglycemia, a recognized cardiovascular risk factor akin to arterial hypertension and obesity
| [6] | Hanley, A. J., Williams, K., Festa, A., Wagenknecht, L. E., D'Agostino, R. B., Kempf, J.,... Haffner, S. M. (2004). Elevations in markers of liver injury and risk of type 2 diabetes: The insulin resistance atherosclerosis study. Diabetes, 53(10), 2623–2632. https://doi.org/10.2337/diabetes.53.10.2623 |
[6]
. The gravitas of T2D lies in its vascular complications, chiefly culminating in severe cardiovascular events such as myocardial infarction (MI) and strokes. Individuals with T2D face a tripled risk of developing cardiovascular diseases, a correlation primarily rooted in chronic hyperglycemia
| [7] | Sharmini, S., Sharif, M. Z., Yeow, T. C., & Ismail, A. A. S. (2014). Risk of cardiovascular events in patients with diabetes mellitus on statins and antihypertensive medications. Current Drug Safety, 9(2), 106–110. https://doi.org/10.2174/15748863113099990032 |
[7]
.
Furthermore, glycated hemoglobin (HbA1C), obesity, and dyslipidemia associated with T2D play pivotal roles in the onset of macro/microangiopathic complications
| [8] | Liu, J., Sempos, C. T., Donahue, R. P., Dorn, J., Trevisan, M., Grundy, S. M.,... Haffner, S. M. (2014). Joint distribution of non-HDL and LDL cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care, 37(11), 3138–3146. https://doi.org/10.2337/dc14-0542 |
[8]
. Recent studies underscore the intricate interplay between triglyceride levels, dyslipidemia, and vascular alterations in T2D populations
| [9] | Yoda, M., Kitano, S., & Uchida, K. (2014). Association between total triglycerides and changes in endothelial function in type 2 diabetes mellitus. Journal of Atherosclerosis and Thrombosis, 21(5), 445–453. https://doi.org/10.5551/jat.20583 |
[9]
. Notably, Constantino et al.
| [10] | Constantino, M. I., Molyneaux, L., Limacher-Gisler, F., Al-Saeed, A., Luo, C., Wu, T.,... Twigg, S. M. (2017). Long-term complications and mortality in young-onset diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care, 40(4), 526–532. https://doi.org/10.2337/dc16-0985 |
[10]
proposed that glucose fluctuations may underlie persistent vascular dysfunction in T2D patients, even with target HbA1c levels. Endothelial dysfunction, a key aspect of vascular complications, has been associated with poor glycemic control and insulin resistance
| [11] | Christen, A. I., Armentano, R. L., Sacanella, E., Santana, D. B., Sanchez, R. A., & Miranda, A. (2010). Association between endothelial dysfunction and cardiovascular outcomes in a diabetic population. Diabetes Research and Clinical Practice, 89(3), e35–e38. https://doi.org/10.1016/j.diabres.2010.04.005 |
| [12] | Czestkowska, E., Talarska, D., Szpakow, A., Kasperczyk, J., Gumprecht, J., & Birkner, E. (2019). Evaluation of endothelial function in patients with type 2 diabetes mellitus. Advances in Experimental Medicine and Biology, 1211, 109–113. https://doi.org/10.1007/978-3-030-32622-5_13 |
[11, 12]
.
Despite recent strides in understanding the pathophysiological mechanisms of vascular events in T2D, a comprehensive elucidation of these intricate relationships remains elusive. Recognizing the complexity, the present study endeavors to contribute to this understanding by investigating the cardiovascular risk among Sub-Saharan individuals with T2D. Additionally, the aim of this work was to explore the potential mechanisms implicated in the pathogenesis of vascular complications in this population. By delving into the intricate web of arterial alterations and their early detection in T2D, this scientific work aspire to shed light on critical facets essential for the primary prevention of macro and microvascular complications associated with T2D.
2. Materials and Methods
Study Design and Participants
The current protocol was conducted by a crossover study involving 36 adult participants with Type 2 Diabetes (T2D) selected from Anti-Diabetic Center in Dakar (age: 43,4 ± 6,7 years, BMI: 25.2 ± 4.1 kg/m2 and sex-ratio M/F: 1) and 36 individuals without T2D (controls: 29.8 ± 7.0 years, BMI: 22.7 ± 3.4 kg/m
2 and sex-ratio: M/F:1). The anthropometric characteristics of study population are presented in
table 1. Smokers, both current and former excluded in the protocol. The study design aimed to investigate the impact of Nitric Oxide (NO) administration on vascular function, assessing outcomes such as diameter size and velocity through Flow Mediated Dilation (FMD) of the brachial artery in the two groups (T2D and control groups). The study design aimed to investigate the impact of Nitric Oxide (NO) administration on vascular function, assessing outcomes such as diameter size and velocity through Flow Mediated Dilation (FMD) of the brachial artery.
All subjects included in the study signed an informed consent form before inclusion and relevant ethic committee approved the protocol (0245/2019/CER/UCAD).
2.1. Data Collection
Subjects were in fasting condition for at least 8 to 12h and data were collected by FMD method in both groups (pre –condition) at seven timepoints: baseline (0 seconds), 5 seconds, 30 seconds, 60 seconds, 90 seconds, 120 seconds, and 600 seconds. Second, to determine the maximum obtainable vasodilator response in T2D patients at the same timepoints, an exogenous NO donor ((
Natispray® 0.3mg/dose trinitrine, manufactured: Teofarma S.r.l. Viale Certosa, S/A 27100 Pavia- Italie) administration was realized by as a single high dose (0.3 mg) of sublingual glyceryl trinitrate. A time interval of 15 minutes after reactive hyperemia (i.e., FMD, pre-condition) and NO administration was observed according to the recommendations of Corretti et al.
| [13] | Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. (2002). Mary C Corretti, Todd J Anderson, Emelia J Benjamin, David Celermajer, Francois Charbonneau, Mark A Creager, John Deanfield, Helmut Drexler, Marie Gerhard-Herman, David Herrington, Patrick Vallance, Joseph Vita, Robert Vogel; International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 16; 39(2): 257-65. https://doi.org/10.1016/s0735-1097(01)01746-6 |
[13]
. Hemodynamic parameters, specifically diameter size (mm) and velocity (cm/s), were measured using brachial artery ultrasonography (Flow Mediated Dilation: FMD) in two conditions (pre and post NO administration). This involved the use of a 10-MHz linear transducer connected to an ultrasound device (DC-6 Mindray).
Participants were positioned in a supine position for 15 minutes in a quiet, temperature-controlled room. The right arm was extended and immobilized at a 60° angle from the trunk. Baseline diameter and velocity measurements were recorded before inducing reactive hyperemia by inflating a cuff to 50 mmHg above systolic blood pressure for 5 minutes. Parameters were then measured at the specified timepoints during rapid cuff deflation. In the research laboratory brachial artery blood flow was measured by the same experienced cardiologist and using ultrasound according to the guidelines described by Corretti et al.
| [13] | Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. (2002). Mary C Corretti, Todd J Anderson, Emelia J Benjamin, David Celermajer, Francois Charbonneau, Mark A Creager, John Deanfield, Helmut Drexler, Marie Gerhard-Herman, David Herrington, Patrick Vallance, Joseph Vita, Robert Vogel; International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 16; 39(2): 257-65. https://doi.org/10.1016/s0735-1097(01)01746-6 |
[13]
and Thijssen et al.
| [14] | Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans (2019). Dick H J Thijssen, Rosa Maria Bruno, Anke C C M van Mil, Sophie M Holder, Francesco Faita, Arno Greyling, Peter L Zock, Stefano Taddei, John E Deanfield, Thomas Luscher, Daniel J Green, Lorenzo Ghiadoni. Eur Heart J. 7; 40(30): 2534-2547. https://doi.org/10.1093/eurheartj/ehz350 |
[14]
and the FMD reproducibility rate was 8-11% between the two measurements
| [15] | Sickle Cell Trait Worsens Oxidative Stress, Abnormal Blood Rheology, and Vascular Dysfunction in Type 2 Diabetes (2015). Mor Diaw, Vincent Pialoux, Cyril Martin, Abdoulaye Samb, Saliou Diop, Camille Faes, Pauline Mury, Niama Sall Diop, Saïd-Norou Diop, Brigitte Ranque, Maïmouna Ndour Mbaye, Nigel S Key, Philippe Connes. Diabetes Care. 38(11): 2120-7. https://doi.org/10.2337/dc15-0699 |
[15]
. All participants refrained from drinking beverages containing caffeine or alcohol for 12 h before the examination and were also advised not to take antihypertensive or vasodilator drugs the day of FMD examination.
2.2. Study Population and Demographic Information
Participants were recruited from individuals with T2D actively receiving care at the Marc Sankale Anti-Diabetic Center (Abass NDAO Hospital, Dakar, Senegal) and control subjects were selected from blood donor population in Dakar. For the T2D population, demographic and clinical information collected at the pre-treatment baseline included age (years), body mass index (BMI), diastolic and systolic blood pressure (mm/Hg), total triglyceride (g/l), creatinine (mg/l), high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels (g/l), years since diabetes diagnosis, and binary indicators of insulin and oral diabetes medication use.
2.3. Variable Selection and Cleaning
There were several variables that were not considered for model building due to the potential for multicollinearity. HbA1C (%) and fasting glucose were highly correlated (Pearson’s r= 0.82) hence fasting glucose was removed from the model. All subjects with hypertension were on antihypertensive medication hence hypertension was kept in place of the indicator for antihypertensive medication use. Diastolic and systolic blood pressure were highly correlated (Pearson’s r= 0.85) but were applied in the calculation of Mean arterial pressure (MAP) (mm/Hg) as follows:
diastolic BP + (systolic- diastolic BP) /3. Low-density lipoprotein and total cholesterol explained most of the variance related to cholesterol hence HDLwas removed. Age and BMI were centered around the mean age (43 years) and mean BMI (25.0), respectively. HbA1c was centered at about 6%, since the normal range for level for hemoglobin A1c is less than 6%. As a comparison to a non-diabetic sample,
table 1 displays the distribution of variables for subjects with (case) and without (control) diabetes while
table 1 shows the distribution of the outcome variables, diameter size and velocity across the varying factors.
2.4. Data Analysis
Due to the repeated measures design of the study and resulting high intra-class correlation coefficient (diameter: 0.48; velocity: 0.25), adjustments for the within-subject correlation of the outcomes taken at the seven timepoints for each subject were made by employing a General Estimating Equation (GEE) regression model with correlation structure, autoregressive-1 (AR-1). AR-1 was chosen based on the assumption that outcome measurements closer in time would be more correlated and that as measurements get farther apart they are less correlated. Though, results remained unchanged when compared to other correlation structures.
Furthermore, time was not linearly correlated with the outcome variables, diameter size and velocity, (
Figure 1) and as expected, attempting to fit a model assuming a linear relationship between the covariates and the outcome variables resulted in poor fit. A log transformation of the outcome variable, diameter size, and a natural log transformation of the second outcome variable, velocity, resulted in the best fit. Consequent to these transformations of the outcome variables, beta coefficients, β1,2,..., that resulted from the GEE models were interpreted as such: (1-e
B1,2,…)*100 so that β1,2,…=1 was equivalent to no association between β1,2,…and diameter size, and every unit above or below 1 meant a 1% increase or decrease change in diameter size, respectively; for the outcome, velocity, beta coefficients were interpreted so that every one-unit increase in β1,2,… results in β1,2,…*100 percent (%) change in velocity. Additionally, all continuous variables were scaled before GEE modeling.
To better understand the impact of the covariates on the relationship between NO administration and diameter size, four models were separately evaluated: 1) an unadjusted model between NO administration status and diameter size; 2) model 1 + age, years since Diabetes diagnosis, BMI, MAP, HbA1c, LDL, total triglyceride, creatinine, and hypertension (reference=no); 3) model 2 + insulin use (reference=no) and oral diabetes medication use (reference=no), and time (seconds) (reference=baseline). Models 1-3 are reported in
table 3. The last model (reported in
table 3) was model 3 + an interaction term, NO administration status x time (to assess the impact of the treatment status on diameter size over time). Identical to the aforementioned models, four additional models were evaluated for the outcome, velocity (
Tables 5 and 6). Robust standard errors were used to calculate 95% confidence intervals (95% CI) for the determination and interpretation of statistical significance (alpha=0.05). All analyses were conducted in the R software (version 3.3.2; “Sincere Pumpkin Patch”).
3. Results
3.1. Table Incorporation
The different results are presented in the tables and figures.
Tables 1 and 2 provided a detailed presentation of participant characteristics, highlighting differences between control and case groups and exploring mean and median values for diameter size and velocity across various covariates. Additionally
Table 3 and
Table 5 presented key results from the GEE models, offering insights into the impact of NO administration and various covariates on diameter size and velocity over time (
Table 4 and
Table 6).
Table 1 presents the characteristics of the study population, comparing individuals with and without diabetes (controls). The variables considered include age, body mass index (BMI), blood pressure, lipid profile, diabetes-related parameters and blood flow (diameter and blood velocity). Notably, individuals with T2D exhibited higher levels of HbA1c, indicative of chronic hyperglycemia, and other metabolic abnormalities.
Additionally,
Table 2 presents the distribution of the outcome variables, diameter size, and velocity across various factors.
3.2. Impact of NO Administration on Vascular Function
Nitric oxide (NO) administration was a central focus of the current study, aimed at understanding its influence on type 2 diabetes-related vascular dysfunction as well as the factors involved in alterations in blood flow. Unadjusted models (not shown) found that pre- NO administration, there was no change in diameter size between baseline and 60 seconds; however, diameter size increased to 2.80% by 90 seconds (compared to baseline) and up to 3.00% from baseline at 120 seconds before returning to baseline levels.
Table 3 outlines the results of GEE models examining the impact of NO administration on the diameter size of the brachial artery. Post-NO administration, participants exhibited a significant increase in diameter size compared to the pre-NO state, ranging from 17% to 20% despite adjusting for other clinically relevant factors. Nevertheless, the beneficial effect of NO administration on diameter size varied over time when it was combined with various clinical and therapeutic such as elevated age (
β=1.09; 95%IC: 1.07, 1.11), increased BMI (
β= 1.03; 95%IC: 1.01, 1.04), LDL (
β=1.16; 95%IC: 1.12, 1.21), creatinine (
β= 1.17 95%IC: 1.12, 1.21), having hypertension (
β= 1.06; 95%IC: 1.03, 1.10)) and insulin use (
β = 1.13; 95%IC 1.10, 1.16), as observed in
Table 3. However increased levels of HbA1C (95% CI: 0.95, 0.98), total cholesterol (95% CI: 0.78, 0.84) and longer years since diabetes diagnosis (95% CI: 0.83, 0.89) were associated with decreased diameter size (3%, 19%, and 14% respectively,
Table 3).
3.3. Velocity Changes and Contributing Factors
Table 5 describes the changes in velocity associated with NO administration and other covariates. Post-NO administration, participants experienced a significant increase in dilation velocity, emphasizing the vasodilatory effect of NO. Interestingly, the relationship between velocity and time exhibited a non-linear pattern, with variations in dilation velocity observed both pre- and post-NO administration.
Factors such as age, BMI, mean arterial pressure (MAP), HbA1c, LDL, insulin use, and hypertension were found to influence velocity changes related to NO administration. For instance, increased age and creatinine levels were associated with increased diameter size, while modifiable factors such as increased LDL level, MAP and insulin use were associated with lowered blood velocity (β=-6.97; 95% CI: -12.23, -1.71, β=-16.21; 95% CI: -30.20, -2.22 and β=-9.82; 95% CI: -13.51, -6.13 respectively).
3.4. Association Between Covariates and Vascular Parameters
To comprehensively understand the impact of various covariates on vascular parameters,
Table 3 and
Table 6 provided detailed insights into the association between different factors and the percentage change in diameter and velocity at different time intervals. This analysis contributes to a nuanced understanding of how age, years since diabetes diagnosis, BMI, MAP, HbA1c, LDL, total triglyceride, creatinine, hypertension, insulin use, and oral diabetes medication use influence vascular dynamics.
4. Discussion
The present study delves into the intricate landscape of vascular complications in Sub-Saharan individuals with Type 2 Diabetes (T2D), shedding light on both prevalence and potential mechanisms. The high prevalence of T2D in Sub-Saharan Africa, as highlighted by the World Health Organization (WHO) and projections by the International Diabetes Federation (IDF), underscores the urgency of understanding the associated vascular complications in this region
| [2] | International Diabetes Federation. (2016). IDF Diabetes Atlas (7th ed.). Retrieved from https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/13-diabetes-atlas-seventh-edition.html |
| [3] | Mbanya, J. C., Motala, A. A., Sobngwi, E., Assah, F. K., Enoru, S. T., & Diabetes in Sub-Saharan Africa Study Group. (2014). Diabetes in sub-Saharan Africa. The Lancet, 383(9933), 1009–1020. https://doi.org/10.1016/S0140-6736(13)62189-7 |
| [4] | World Health Organization. (2014). Global status report on noncommunicable diseases 2014. Retrieved from https://www.who.int/nmh/publications/ncd-status-report-2014/en/ |
[2-4]
.
The vascular complications observed in T2D often manifest as cardiovascular events, including myocardial infarction and stroke. This results align with existing literature, emphasizing the threefold increase in the risk of cardiovascular diseases in T2D patients
| [7] | Sharmini, S., Sharif, M. Z., Yeow, T. C., & Ismail, A. A. S. (2014). Risk of cardiovascular events in patients with diabetes mellitus on statins and antihypertensive medications. Current Drug Safety, 9(2), 106–110. https://doi.org/10.2174/15748863113099990032 |
[7]
. Crucially, chronic hyperglycemia emerges as a linchpin in this association, highlighting the imperative need for effective glycemic control in managing and preventing vascular complications.
The current exploration of potential mechanisms contributing to vascular complications in sub-Saharan T2D individuals uncovers the intricate interplay of various clinical and therapeutic factors. The role of insulin resistance leading to hyperinsulinism and chronic hyperglycemia in the risk of cardiovascular complications has been described with established pathways
| [6] | Hanley, A. J., Williams, K., Festa, A., Wagenknecht, L. E., D'Agostino, R. B., Kempf, J.,... Haffner, S. M. (2004). Elevations in markers of liver injury and risk of type 2 diabetes: The insulin resistance atherosclerosis study. Diabetes, 53(10), 2623–2632. https://doi.org/10.2337/diabetes.53.10.2623 |
[6]
. Moreover, the influence of glycated hemoglobin (HbA1C), obesity, and dyslipidemia on macro/microangiopathic complications aligns with contemporary research
| [8] | Liu, J., Sempos, C. T., Donahue, R. P., Dorn, J., Trevisan, M., Grundy, S. M.,... Haffner, S. M. (2014). Joint distribution of non-HDL and LDL cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care, 37(11), 3138–3146. https://doi.org/10.2337/dc14-0542 |
[8]
. The modifiability of obesity as a determinant of vascular dysfunction, independent of other traditional risk factors, as highlighted by Liu et al.
| [8] | Liu, J., Sempos, C. T., Donahue, R. P., Dorn, J., Trevisan, M., Grundy, S. M.,... Haffner, S. M. (2014). Joint distribution of non-HDL and LDL cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care, 37(11), 3138–3146. https://doi.org/10.2337/dc14-0542 |
[8]
, underscores the potential for targeted interventions in T2D populations.
The present work underscores the importance of understanding the temporal dynamics of vascular alterations considering modifiable clinical and therapeutic factors. The significance of glucose fluctuations, even within target HbA1c levels, as elucidated by Constantino et al.
| [10] | Constantino, M. I., Molyneaux, L., Limacher-Gisler, F., Al-Saeed, A., Luo, C., Wu, T.,... Twigg, S. M. (2017). Long-term complications and mortality in young-onset diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care, 40(4), 526–532. https://doi.org/10.2337/dc16-0985 |
[10]
, underscores the need for nuanced glycemic control strategies. Additionally, the association between poor glycemic control, insulin resistance, and endothelial dysfunction, in line with Yoda et al.
| [9] | Yoda, M., Kitano, S., & Uchida, K. (2014). Association between total triglycerides and changes in endothelial function in type 2 diabetes mellitus. Journal of Atherosclerosis and Thrombosis, 21(5), 445–453. https://doi.org/10.5551/jat.20583 |
[9]
emphasizes the multifaceted nature of T2D-related vascular complications. The duration of diabetes and persistent hyperglycemia emerge as critical determinants of endothelial function alterations
| [11] | Christen, A. I., Armentano, R. L., Sacanella, E., Santana, D. B., Sanchez, R. A., & Miranda, A. (2010). Association between endothelial dysfunction and cardiovascular outcomes in a diabetic population. Diabetes Research and Clinical Practice, 89(3), e35–e38. https://doi.org/10.1016/j.diabres.2010.04.005 |
[11]
, urging early detection and intervention to mitigate the long-term impact of T2D on vascular health.
The comprehensive examination of various covariates in this study provides valuable insights into their individual and collective impact on vascular outcomes after NO administration. The notable increase in diameter size post-Nitric Oxide (NO) administration, even after adjusting for clinically relevant factors, suggests a potential avenue for therapeutic interventions. However, the beneficial effect of NO could be influenced by other factors such as the age of the diabetic patient, elevated creatinine levels and insulin use, each of which has a different impact on NO-related improvement in vascular function. In addition, arterial hypertension, increased low-density lipoprotein (LDL) levels and a body mass index (BMI) greater than 25.0 also appear to be factors that contribute negatively to NO-related blood flow enhancement in the type 2 diabetic population. The nuanced impact of these factors necessitates tailored approaches in managing T2D patients.
The non-linear relationship between time and vascular outcomes, as observed in this work, emphasizes the dynamic nature of vascular alterations in T2D. The sustained increase in diameter size post-NO administration indicates the potential benefits of targeted interventions. The fact that blood flow improvement observed after NO administration seems changed by modifiable clinic-therapeutic factors such HbA1C levels, total cholesterol, and years since diabetes diagnosis, further emphasizes the need for holistic management strategies.
This scientific work, with its focus on Sub-Saharan African individuals with T2D, contributes to the growing body of literature on the global burden of diabetes. The nuanced exploration of vascular complications and their potential mechanisms in this population provides context-specific insights crucial for tailored healthcare strategies. However, the study has limitations, including a relatively small sample size and the absence of a non-diabetic control group. Future research with larger cohorts and diverse control groups could further enhance the understanding of the intricate relationships between T2D and vascular complications.
In conclusion, the present findings underscore the pervasive impact of T2D on vascular health in Sub-Saharan African individuals. The intricate web of factors contributing to vascular complications necessitates a personalized multifaceted approach to type 2 diabetes management. Targeted interventions, addressing both traditional and novel risk factors, hold promise in mitigating the burden of T2D-related vascular events. As the protocol strives for a comprehensive understanding of the intricate pathways linking T2D and vascular complications, the present study contributes valuable insights to inform both clinical practice and public health individualized strategies in the Sub-Saharan context.
5. Strengths and Limitations
Contextual Relevance: current study uniquely focuses on Sub-Saharan African individuals with Type 2 Diabetes (T2D), providing valuable insights into the vascular complications within this specific population. This context-specific approach contributes to a more nuanced understanding of the global impact of diabetes. Comprehensive Assessment: The study incorporates a thorough examination of various covariates, including age, BMI, glycemic control, and medication use on beneficial effect of NO on vascular complications related to type 2 diabetes. This comprehensive approach allows for a more holistic understanding of the factors influencing vascular outcomes in individuals with T2D. Temporal Dynamics Exploration: By assessing vascular outcomes at multiple timepoints and considering the impact of Nitric Oxide (NO) administration, this study delves into the temporal dynamics of vascular alterations. This nuanced exploration enhances the understanding of the evolving nature of vascular complications in T2D. Clinical Relevance: The findings regarding the potential benefits of NO administration and the impact of various covariates on vascular hemodynamic function provide clinically relevant information. These insights could guide targeted interventions and personalized treatment strategies for individuals with T2D.
6. Limitations
Sample Size: The study is relatively small sample size may limit the generalizability of the findings. Future research with larger cohorts would strengthen the robustness and external validity of the results. Absence of a Control Group: The lack of a non-diabetic control group during the NO administration period hinders the ability to compare vascular outcomes in individuals with T2D to those without diabetes. Including a control group would provide a baseline for understanding the specific impact of T2D on vascular health. A more diverse and multicenter approach would enhance the study's representativeness. Cross-Sectional Design: The cross-sectional nature of the study limits the establishment of causal relationships. Longitudinal studies could provide insights into the temporal evolution of vascular complications and the efficacy of interventions over time. Limited Mechanistic Insights: While the study explores potential mechanisms contributing to vascular complications, the complexity of these mechanisms requires more in-depth investigations. Further research could elucidate the underlying pathophysiological processes with greater precision. External Validity: The findings may be specific to the Sub-Saharan African population and may not fully generalize to other ethnic or geographical groups. Caution should be exercised when extrapolating the results to broader populations.
Despite these limitations, this scientific work study lays the groundwork for future research endeavors and highlights the importance of tailored interventions in managing vascular complications in individuals with T2D in Sub-Saharan Africa.
7. Conclusion
In conclusion, the investigation into vascular complications in individuals from Sub-Saharan Africa with Type 2 Diabetes (T2D) unfolds several pivotal revelations, offering insights that warrant careful consideration and future exploration. Firstly, these findings highlight the potential significance of Nitric Oxide (NO) administration on vascular/endothelial function among individuals with T2D. This observation suggests a promising avenue for personalized therapeutic interventions aimed at improving vascular health in this specific population. Secondly, the meticulous temporal analysis of vascular outcomes, both pre- and post-NO administration, provides a nuanced understanding of how vascular parameters evolve over time. This temporal insight contributes to a more thorough characterization of disease progression, an essential aspect for devising effective interventions. Thirdly, the present study underscores the influence of various covariates, including age, BMI, glycemic control, and medication use, on vascular outcomes. This emphasizes the multifaceted nature of vascular complications in T2D, highlighting the need for personalized and holistic approaches to patient care. Fourthly, the clinical implications of identifying factors contributing to vascular dysfunction in individuals with T2D are significant. Healthcare practitioners can leverage this information to tailor interventions, optimize glycemic control, and address modifiable risk factors to mitigate the impact of diabetes-related vascular events. Fifthly, while this study contributes valuable insights, it also underscores the need for further research. Larger and more diverse cohorts, longitudinal studies, and in-depth mechanistic investigations are warranted to validate and extend the findings of this study. Additionally, research exploring the generalizability of these results to other populations is paramount.
In essence, this structured exploration contributes to the expanding body of knowledge on T2D-related vascular complications, particularly in the understudied context of Sub-Saharan Africa. The identified associations and potential benefits of NO administration open avenues for future research and therapeutic exploration. Ultimately, the findings of this protocol accentuate the urgency of comprehensive and tailored strategies to address the mounting burden of T2D-associated vascular complications in this population.
Author Contributions
Mor Diaw: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Wrating- Review & Editing
Awa Ba Diop: Investigation, Methodology, Writing- original draft
Lorinette Wirth: Conceptualization, Formal Analysis, Writing- original draft, Wrating- Review & Editing
Abdou Khadir Sow: Data curation, Formal Analysis, Investigation
Jean Fidèle Nnang Essone: Writing- original draft, Writing – review & editing
Demba Diedhiou: Data curation, Methodology, Validation
Djiby Sow: Data curation, Methodology, Validation
Aissatou Seck/Diop: Data curation, Methodology, Validation
Salimata Houndjo Diagne: Data curation, Methodology, Validation
Maimouna Toure: Data curation, Methodology, Validation, Writing- original draft
Maimouna Ndour/Mbaye: Investigation, Methodology, Writing- original draft
Abdoulaye Ba: Validation, Writing- original draft, Writing – review & editing
Abdoulaye Samb: Validation, Writing- original draft, Writing – review & editing
Bamba Gaye: Formal Analysis, Writing- original draft, Writing – review & editing
Rhonda Belue: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing – review & editing
Acknowledgments
The authors would thank all patients who accepted to participate in the present study.
Funding Information
No funding for this study.
Ethics Statement
Ethic committee approved the protocol.
Data Availability Statement
The data will be provided on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
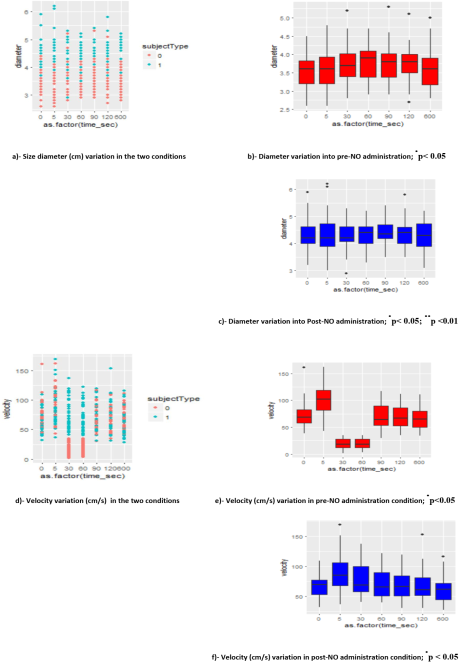
Figure 1. Diameter and velocity variations in different times and in two conditions (pre and post NO administration).
Sujet 0: pre-condition - Sujet 1: Post NO administration condition
Difference from baseline time: p< 0.05; p <0.01
Table 1. Median (range) anthropometric, biochemical and hemodynamic characteristics, in the two groups.
Control | Case |
Combined | Pre-NO | Post-NO |
Age (yrs) | 28.0 (17-42) | 45 (30-50) | | |
BMI (kg/m2) | 22.5 (17.1-31.2) | 24.6 (18.4-32.2) | | |
MAP (mm/Hg) | 132.2 (108.3, 153.3) | 140 (110, 208.33) | | |
LDL (g/l) | 1.21 (0.77, 2.47) | 1.29 (0.58-2.62) | | |
Triglyceride (g/l) | 0.64 (0.28, 1.38) | 0.89 (0.38-2.34) | | |
HbA1c (%) | 4.55 (3.12, 9.04) | 7.55 (4.9-16.4) | | |
Diameter (mm) | 3.8 (2.8, 5) | 4 (2.6-6.2) | 3.7 (2.6, 5.3) | 4.3 (2.9, 6.2) |
Velocity (cm/s) | 67.5 (18, 102) | 65 (2-169) | 61.5 (2, 162) | 67.5 (28, 169) |
Table 2. Mean (standard deviation) diameter (mm) and velocity (cm/s) by covariates (n=36).
NO administration | Diameter | Velocity |
Yes | 4.34 (0.53) | 59.88 (33.64) |
No | 3.67 (0.51) | 72.18 (25.22) |
Time (seconds) | | |
0 | 3.93 (0.66) | 70.35 (21.05) |
5 | 3.98 (0.71) | 93.82 (27.66) |
30 | 4.01 (0.61) | 48.15 (34.99) |
60 | 4.05 (0.54) | 44.49 (31.09) |
90 | 4.09 (0.58) | 71.26 (22.16) |
120 | 4.07 (0.57) | 69.74 (23.52) |
600 | 3.93 (0.64) | 64.42 (20.84) |
Age (years) | | |
< 45 (n=15) | 3.95 (0.65) | 64.85 (31.01) |
≥ 45 (n=21) | 4.04 (0.59) | 66.84 (29.87) |
Years since diabetes dx | | |
<7 | 4.03 (0.65) | 63.35 (28.98) |
≥7 | 3.87 (0.56) | 70.25 (31.96) |
BMI (kg/m²) | | |
< 25 (n=19) | 3.90 (0.57) | 65.53 (30.00) |
≥ 25 (n=17) | 4.13 (0.64) | 66.60 (30.75) |
MAP (mm/Hg) | | |
110-150 (n=26) | 3.99 (0.64) | 64.07 (29.19) |
>150 (n=10) | 4.06 (0.56) | 71.14 (32.68) |
HbA1c (%) | | |
<7 (n=11) | 4.08 (0.67) | 69.38 (29.03) |
≥7 (n=25) | 3.98 (0.59) | 65.56 (30.81) |
LDL (g/l) | | |
<1.3 (n=18) | 4.06 (0.66) | 69.76 (31.31) |
1.3-1.89 (n=13) | 3.94 (0.57) | 60.82 (27.97) |
≥1.9 (n=5) | 4.02 (0.56) | 66.16 (31.09) |
Total triglyceride (g/l) | | |
<1.50 (n=33) | 4.03 (0.60) | 66.89 (30.90) |
≥1.50 (n=3 | 3.8 (0.74) | 55.57 (20.79) |
Creatinine (mg/l) | | |
<11 (n=29) | 3.99 (0.61) | 67.20 (30.54) |
>11 (n=7) | 4.07 (0.65) | 61.20 (29.10) |
Hypertension | | |
Yes (n=8) | 4.12 (0.54) | 74.40 (31.83) |
No (n=20) | 3.96 (0.63) | 62.21 (28.81) |
Insulin | | |
Yes (n=15) | 4.04 (0.65) | 63.28 (32.05) |
No (n=21) | 3.98 (0.57) | 68.00 (28.94) |
Diabetes medication (oral) | | |
Yes (n=30) | 4.03 (0.64) | 65.86 (29.37) |
No (n=6) | 3.91 (0.45) | 66.90 (34.94) |
Table 3. Results from GEE model examining the impact of NO administration on % mm change in diameter (95%CI).
| Model 1 | Model 2 | Model 3 |
Post NO administration (ref=pre) | 1.18 (1.17, 1.20) | 1.18 (1.17, 1.20) | 1.18 (1.17, 1.20) |
Time (seconds) (ref= baseline) | | | |
5 | | | 1.01 (0.98, 1.07) |
30 | | | 1.03 (1.00, 1.07) |
60 | | | 1.04 (1.00, 1.07) |
90 | | | 1.05 (1.01, 1.09) |
120 | | | 1.04 (1.01, 1.08) |
600 | | | 1.00 (0.96, 1.04) |
aAge (years) | | 1.05 (1.04, 1.07) | 1.09 (1.07, 1.11) |
Years since Diabetes dx | | 0.92 (0.90, 0.94) | 0.86 (0.83, 0.89) |
bBMI (kg/m2) | | 1.97 (0.59, 3.34) | 1.03 (1.01, 1.04) |
Mean Arterial Pressure (mm/Hg) | | 1.00 (0.89, 1.11) | 1.05 (0.95, 1.16) |
cHbA1c (%) | | 0.98 (0.96, 1.00) | 0.97 (0.95, 0.98) |
LDL (g/l) | | 1.12 (1.08, 1.16) | 1.16 (1.12, 1.21) |
Total cholesterol (g/l) | | 0.85 (0.82, 0.88) | 0.81 (0.78, 0.84) |
Creatinine (mg/l) | | 1.19 (1.15, 1.23) | 1.17 (1.12, 1.21) |
Hypertension (ref=no) | | 1.08 (1.04, 1.12) | 1.06 (1.03, 1.10) |
Insulin (ref=no) | | | 1.13 (1.10, 1.16) |
Diabetes medication (oral) (ref=no) | | | 1.03 (1.00, 1.07) |
Bold font signifies statistical significance at alpha=0.05
Negative values (-) indicate decrease in diameter size
aCentered around mean, 43 years.
bCentered around mean, 25.
cCentered around 6%.
Table 4. Change of diameter size (from baseline: 3.52 cm) in the two condition (pre-NO and post NO administration).
Time (seconds) | Pre-NO Diameter size (% change from baseline) | Post-NO Diameter size (% change from baseline) |
5 | 3.6 (1.02) | 4.36 (1.01) |
30 | 3.72 (1.06) | 4.31 (1.00) |
60 | 3.75 (1.07) | 4.34 (1.01) |
90 | 3.76 (1.07) | 4.41 (1.02) |
120 | 3.77 (1.07) | 4.36 (1.01) |
600 | 3.58 (1.02) | 4.30 (0.99) |
Table 5. Results from GEE model examining the impact of NO administration on % change in blood velocity (cm/s) (95%CI).
| Model 1 | Model 2 | Model 3 |
Post NO administration (ref=pre) | 16.24 (11.64, 20.84) | 16.24 (11.64, 20.84) | 16.24 (11.64, 20.84) |
Time (seconds) (ref= baseline) | | | |
5 | | | 12.34 (8.00, 16.70) |
30 | | | -29.81 (-35.29, -24.53) |
60 | | | -31.72 (-37.66, -25.77) |
90 | | | 0.24 (-4.34, 4.83) |
120 | | | -0.87 (-5.41, 3.67) |
600 | | | -4.26 (-8.82, 0.30) |
aAge | | -0.52 (-0.3.84, 2.80) | -3.73 (-6.01, -1.45) |
Years since Diabetes dx | | -0.65 (-6.58, 5.28) | 6.83 (2.87, 10.79) |
bBMI | | 1.38 (-1.25, 4.01) | 0.84 (-6.12, 2.30) |
Mean Arterial Pressure (mm/Hg) | | -10.09 (-32.46, 12.28) | -16.21 (-30.20, -2.22) |
cHbA1c (%) | | -2.54 (-6.25, 1.18) | -1.79 (-3.88, 0.31) |
LDL (g/l) | | -2.71 (-12.17, 6.75) | -6.97 (-12.23, -1.71) |
Total Triglyceride (g/l) | | -0.63 (-8.07, 6.81) | 4.99 (0.13, 9.85) |
Creatinine (mg/l) | | 2.26 (-6.95, 11.48) | 4.74 (-1.32, 10.80) |
Hypertension (ref=no) | | 12.41 (3.10, 21.71) | 13.64 (8.06, 19.22) |
Insulin (ref=no) | | | -9.82 (-13.51, -6.13) |
Diabetes medication (oral) (ref=no) | | | 1.54 (-3.78, 6.87) |
Bold font signifies statistical significance at alpha=0.05
Negative values (-) indicate decrease in diameter size
aCentered around mean, 43 years.
bCentered around mean, 25.
cCentered around 6%.
Table 6. % change in blood velocity compared to baseline across time (73.44 cm/s).
| Pre-NO | Post-NO |
Time (seconds) | | |
5 | 12.45 (7.43, 17.47) | 12.26 (1.41, 23.11) |
30 | -65.28 (-75.94, -54.63) | 5.46 (-18.15, 29.07) |
60 | -64.46 (-74.76, -54.16) | 1.03 (-20.70, 22.76) |
90 | -1.21 (-6.19, 3.95) | 1.61 (-8.29, 11.51) |
120 | -1.31 (-6.25, 3.62) | -0.43 (-10.49, 9.63) |
600 | -4.15 (-9.19, 0.89) | -4.37 (-14.59, 5.85) |
References
| [1] |
International Diabetes Federation. (2013). IDF Diabetes Atlas (6th ed.). Retrieved from
https://www.idf.org/e-library/epidemiology-research/diabetes-atlas.html
|
| [2] |
International Diabetes Federation. (2016). IDF Diabetes Atlas (7th ed.). Retrieved from
https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/13-diabetes-atlas-seventh-edition.html
|
| [3] |
Mbanya, J. C., Motala, A. A., Sobngwi, E., Assah, F. K., Enoru, S. T., & Diabetes in Sub-Saharan Africa Study Group. (2014). Diabetes in sub-Saharan Africa. The Lancet, 383(9933), 1009–1020.
https://doi.org/10.1016/S0140-6736(13)62189-7
|
| [4] |
World Health Organization. (2014). Global status report on noncommunicable diseases 2014. Retrieved from
https://www.who.int/nmh/publications/ncd-status-report-2014/en/
|
| [5] |
Emerging Risk Factors Collaboration. (2010). Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. The Lancet, 375(9733), 2215–2222.
https://doi.org/10.1016/S0140-6736(10)60484-9
|
| [6] |
Hanley, A. J., Williams, K., Festa, A., Wagenknecht, L. E., D'Agostino, R. B., Kempf, J.,... Haffner, S. M. (2004). Elevations in markers of liver injury and risk of type 2 diabetes: The insulin resistance atherosclerosis study. Diabetes, 53(10), 2623–2632.
https://doi.org/10.2337/diabetes.53.10.2623
|
| [7] |
Sharmini, S., Sharif, M. Z., Yeow, T. C., & Ismail, A. A. S. (2014). Risk of cardiovascular events in patients with diabetes mellitus on statins and antihypertensive medications. Current Drug Safety, 9(2), 106–110.
https://doi.org/10.2174/15748863113099990032
|
| [8] |
Liu, J., Sempos, C. T., Donahue, R. P., Dorn, J., Trevisan, M., Grundy, S. M.,... Haffner, S. M. (2014). Joint distribution of non-HDL and LDL cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care, 37(11), 3138–3146.
https://doi.org/10.2337/dc14-0542
|
| [9] |
Yoda, M., Kitano, S., & Uchida, K. (2014). Association between total triglycerides and changes in endothelial function in type 2 diabetes mellitus. Journal of Atherosclerosis and Thrombosis, 21(5), 445–453.
https://doi.org/10.5551/jat.20583
|
| [10] |
Constantino, M. I., Molyneaux, L., Limacher-Gisler, F., Al-Saeed, A., Luo, C., Wu, T.,... Twigg, S. M. (2017). Long-term complications and mortality in young-onset diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care, 40(4), 526–532.
https://doi.org/10.2337/dc16-0985
|
| [11] |
Christen, A. I., Armentano, R. L., Sacanella, E., Santana, D. B., Sanchez, R. A., & Miranda, A. (2010). Association between endothelial dysfunction and cardiovascular outcomes in a diabetic population. Diabetes Research and Clinical Practice, 89(3), e35–e38.
https://doi.org/10.1016/j.diabres.2010.04.005
|
| [12] |
Czestkowska, E., Talarska, D., Szpakow, A., Kasperczyk, J., Gumprecht, J., & Birkner, E. (2019). Evaluation of endothelial function in patients with type 2 diabetes mellitus. Advances in Experimental Medicine and Biology, 1211, 109–113.
https://doi.org/10.1007/978-3-030-32622-5_13
|
| [13] |
Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. (2002). Mary C Corretti, Todd J Anderson, Emelia J Benjamin, David Celermajer, Francois Charbonneau, Mark A Creager, John Deanfield, Helmut Drexler, Marie Gerhard-Herman, David Herrington, Patrick Vallance, Joseph Vita, Robert Vogel; International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 16; 39(2): 257-65.
https://doi.org/10.1016/s0735-1097(01)01746-6
|
| [14] |
Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans (2019). Dick H J Thijssen, Rosa Maria Bruno, Anke C C M van Mil, Sophie M Holder, Francesco Faita, Arno Greyling, Peter L Zock, Stefano Taddei, John E Deanfield, Thomas Luscher, Daniel J Green, Lorenzo Ghiadoni. Eur Heart J. 7; 40(30): 2534-2547.
https://doi.org/10.1093/eurheartj/ehz350
|
| [15] |
Sickle Cell Trait Worsens Oxidative Stress, Abnormal Blood Rheology, and Vascular Dysfunction in Type 2 Diabetes (2015). Mor Diaw, Vincent Pialoux, Cyril Martin, Abdoulaye Samb, Saliou Diop, Camille Faes, Pauline Mury, Niama Sall Diop, Saïd-Norou Diop, Brigitte Ranque, Maïmouna Ndour Mbaye, Nigel S Key, Philippe Connes. Diabetes Care. 38(11): 2120-7.
https://doi.org/10.2337/dc15-0699
|
Cite This Article
-
APA Style
Diaw, M., Diop, A. B., Wirth, L., Sow, A. K., Essone, J. F. N., et al. (2024). Deciphering Vascular Dynamics Alterations in Sub-Saharan Individuals with Type 2 Diabetes: Overview and Temporal Analysis of Nitric Oxide Administration. Advances in Applied Physiology, 9(1), 1-12. https://doi.org/10.11648/j.aap.20240901.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Diaw, M.; Diop, A. B.; Wirth, L.; Sow, A. K.; Essone, J. F. N., et al. Deciphering Vascular Dynamics Alterations in Sub-Saharan Individuals with Type 2 Diabetes: Overview and Temporal Analysis of Nitric Oxide Administration. Adv. Appl. Physiol. 2024, 9(1), 1-12. doi: 10.11648/j.aap.20240901.11
Copy
|
Download
AMA Style
Diaw M, Diop AB, Wirth L, Sow AK, Essone JFN, et al. Deciphering Vascular Dynamics Alterations in Sub-Saharan Individuals with Type 2 Diabetes: Overview and Temporal Analysis of Nitric Oxide Administration. Adv Appl Physiol. 2024;9(1):1-12. doi: 10.11648/j.aap.20240901.11
Copy
|
Download
-
@article{10.11648/j.aap.20240901.11,
author = {Mor Diaw and Awa Ba Diop and Lorinette Wirth and Abdou Khadir Sow and Jean Fidèle Nnang Essone and Demba Diedhiou and Djiby Sow and Aissatou Seck/Diop and Salimata Houndjo Diagne and Maimouna Toure and Maimouna Ndour/Mbaye and Abdoulaye Ba and Abdoulaye Samb and Bamba Gaye and Rhonda Belue},
title = {Deciphering Vascular Dynamics Alterations in Sub-Saharan Individuals with Type 2 Diabetes: Overview and Temporal Analysis of Nitric Oxide Administration
},
journal = {Advances in Applied Physiology},
volume = {9},
number = {1},
pages = {1-12},
doi = {10.11648/j.aap.20240901.11},
url = {https://doi.org/10.11648/j.aap.20240901.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.aap.20240901.11},
abstract = {Background: Early detection of arterial damage is essential for the primary prevention of complications linked to type 2 diabetes (T2D). The study assessed the cardiovascular risk of sub-Saharan African individuals with T2D, while exploring possible mechanisms involved in the pathogenesis of vascular complications in this population. Methodology: A crossover study of 72 sub-Saharan African adults (36 with T2D and 36 without T2D) was conducted. Outcomes including diameter size (mm) and blood velocity (cm/s) of the brachial artery, were obtained at seven time points: baseline and from 5 seconds to 600 seconds in two conditions: pre- and post Nitric Oxide (NO) administration. HbA1C, fasting glucose, age, BMI, mean arterial pressure (MAP), lipid profile, T2D duration since diagnosis, and binary indicators of insulin and oral diabetes medication were evaluated. Results: NO improved the blood flow compared to the pre-NO after adjustment for clinical factors. The beneficial effect of NO administration on vascular dynamics was influenced by age (B=1.09; 95%IC: 1.07, 1.11), increased BMI (B= 1.03; 95%IC: 1.01, 1.04) and insulin use (B = 1.13; 95%IC 1.10, 1.16). Conclusion: The nuanced impact of these factors on blood flow improvement related to NO necessitates tailored and personalized approaches in managing T2D patients.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Deciphering Vascular Dynamics Alterations in Sub-Saharan Individuals with Type 2 Diabetes: Overview and Temporal Analysis of Nitric Oxide Administration
AU - Mor Diaw
AU - Awa Ba Diop
AU - Lorinette Wirth
AU - Abdou Khadir Sow
AU - Jean Fidèle Nnang Essone
AU - Demba Diedhiou
AU - Djiby Sow
AU - Aissatou Seck/Diop
AU - Salimata Houndjo Diagne
AU - Maimouna Toure
AU - Maimouna Ndour/Mbaye
AU - Abdoulaye Ba
AU - Abdoulaye Samb
AU - Bamba Gaye
AU - Rhonda Belue
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.aap.20240901.11
DO - 10.11648/j.aap.20240901.11
T2 - Advances in Applied Physiology
JF - Advances in Applied Physiology
JO - Advances in Applied Physiology
SP - 1
EP - 12
PB - Science Publishing Group
SN - 2471-9714
UR - https://doi.org/10.11648/j.aap.20240901.11
AB - Background: Early detection of arterial damage is essential for the primary prevention of complications linked to type 2 diabetes (T2D). The study assessed the cardiovascular risk of sub-Saharan African individuals with T2D, while exploring possible mechanisms involved in the pathogenesis of vascular complications in this population. Methodology: A crossover study of 72 sub-Saharan African adults (36 with T2D and 36 without T2D) was conducted. Outcomes including diameter size (mm) and blood velocity (cm/s) of the brachial artery, were obtained at seven time points: baseline and from 5 seconds to 600 seconds in two conditions: pre- and post Nitric Oxide (NO) administration. HbA1C, fasting glucose, age, BMI, mean arterial pressure (MAP), lipid profile, T2D duration since diagnosis, and binary indicators of insulin and oral diabetes medication were evaluated. Results: NO improved the blood flow compared to the pre-NO after adjustment for clinical factors. The beneficial effect of NO administration on vascular dynamics was influenced by age (B=1.09; 95%IC: 1.07, 1.11), increased BMI (B= 1.03; 95%IC: 1.01, 1.04) and insulin use (B = 1.13; 95%IC 1.10, 1.16). Conclusion: The nuanced impact of these factors on blood flow improvement related to NO necessitates tailored and personalized approaches in managing T2D patients.
VL - 9
IS - 1
ER -
Copy
|
Download